Webinar — Live Tour With The Happy Tree — Psychiatry and De-addiction Hospital
The following blog has been reviewed by a Psychologist. If you are reading the blog on a mobile phone, you can see the reviewer’s profile at the end of the blog. Please see our editorial policy here.
In our weekly webinars, we talk about various industry scenarios and challenges of rehabs across the country, along with the de-addiction and mental health challenges faced by the mental health community and people in general.
In the 11th webinar of the series, we invited Dr Anuneet Sabharwal from The Happy Tree. The webinar was hosted by Mr Vikram Kumar – Managing Director of RehabPath, India. In the webinar, Dr Sabharwal gave a live tour of The Happy Tree, a psychiatric and de-addiction hospital in Delhi.
In this blog, you can read the summary of the webinar, or you can watch it online here.
Vikram: Please tell us about yourself and The Happy Tree facility.
Dr Anuneet Sabharwal: I’m a Delhi-based psychiatrist. I’ve been in the business of mental health, addiction, and psychosexual health for the last ten years. I’ve been practising for the last four to five years. Constructing The Happy Tree hospital took me four years and the journey has been a roller coaster ride. I’m proud of the fact that I built this facility from scratch. The struggles I had were in terms of psychiatric setups like patient to bed ratio, patient to nurse ratio, or patient to doctor ratio, including the space for patients, activities, and their safety.
We made sure that there are no pro-suicidal construction glitches in place and the environment isn’t too stimulating for patients. We took care of everything that is required for a psychiatric hospital to function properly during the construction process.
Some of the struggles I faced were with the application categories in which I could apply for approval of my facility from the government. I applied for the comprehensive psychiatric hospital category, of which de-addiction is a part. If you are a de-addiction centre owner and not a doctor yourself, you cannot apply to this category.
Vikram: From here, can we please move onto your facility’s tour and get an idea from a doctor’s perspective?

This is an escape route. It is only to be used in exceptional cases when the patient gets violent. Hence, the door for the route is always unlocked. It is not visible to anyone else in the building as it is exclusive to the doctor or the therapist. I believe it is not usually a part of other such setups.

We are now in the open OPD area. I will brief you on the various rooms we have in the facility.
We have a family therapy room. There is a procedure room where many procedures are given to the patient. We have recliners for every procedure. The patients are free to switch the lights off or put on the AC during the procedures.
I will tell you about the different kinds of procedures we practice in the facility and how we differ from other facilities.
One of the guidelines for a psychiatric hospital facility is to have a diagnostic lab. We have a tie-up with SRL for this. They have a collection centre inside our facility. It is essential for patients who come with an overdose or acute withdrawal symptom.

This is the main counselling room for the OPD centre. We have two recliners here because couples also come for therapy.
I will also brief you on some of the devices we use during psychotherapy, which is referred to as assisted psychotherapy.

These devices are used for clinical purposes all across the world. This is a CES device or Cranial Electrotherapy Stimulation device. It is attached to both earlobes with the help of a clip. This is usually worn during the psychotherapy session for about 15-20 minutes, which enhances the effect of therapy.

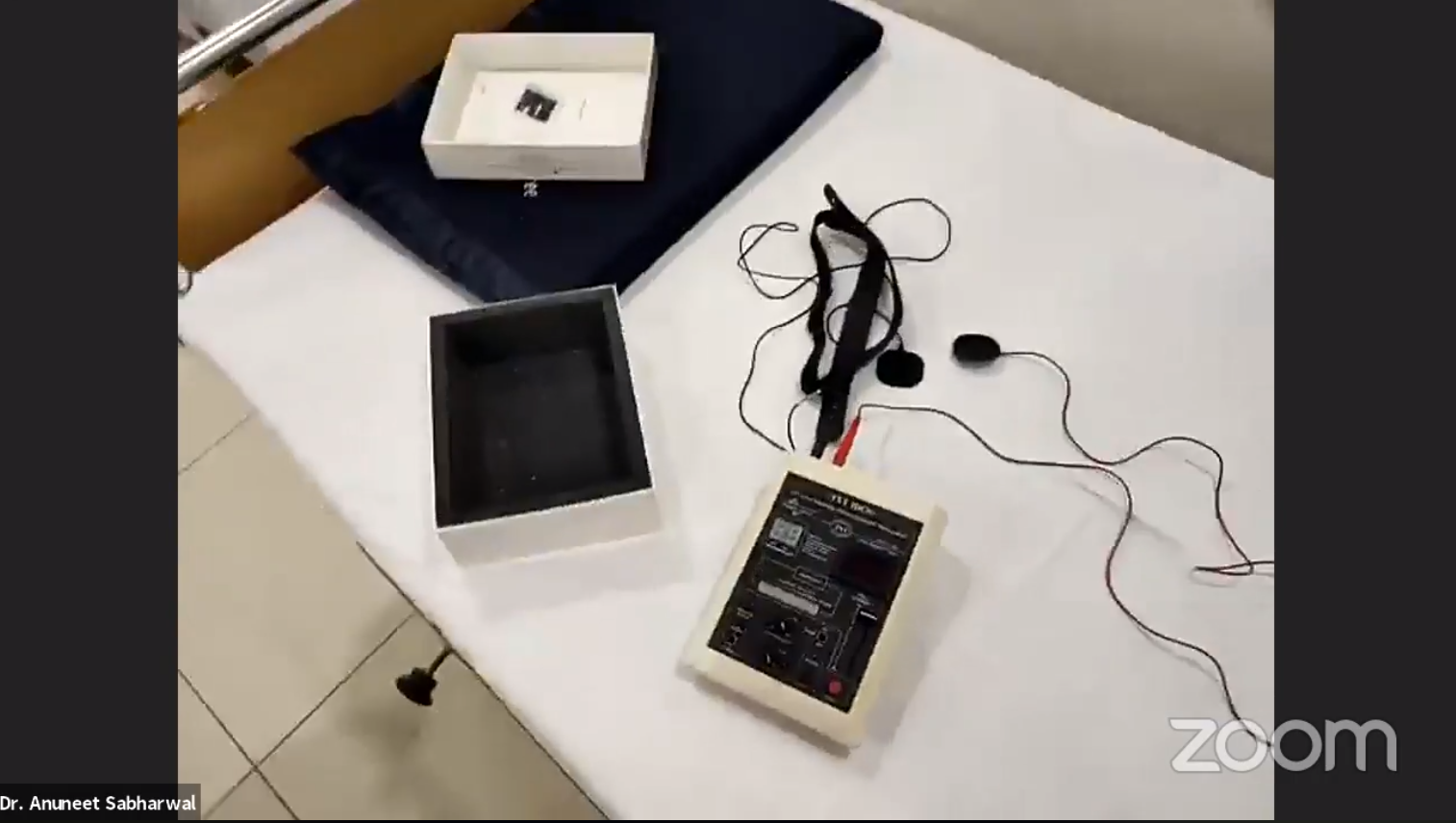
This device is called an Audio-Visual Entrainment Device connected with the help of a couple of clips to your earlobes. It comes with a set of earphones for audio entrainment and a pair of glasses that are used for Visual Entrainment. These glasses emit a unique set of lights when switched on and help entrain the human brain.
It is also sometimes paired with psychotherapy, where a person is given half an hour of counseling and half an hour of the Audio-Visual Entrainment. The sessions can vary between 40, 80, 120 or sometimes 180 minutes, depending upon the severity of the patient’s condition.

This is a Russian device called Transcranial Pulsed Electromagnetic Field (TPEMF) therapy device. It is connected to the patient’s head, attached to the temples. This device requires a session of a minimum of about 20 minutes, and we usually make it a 40 minutes session. It is used for insomnia, anxiety, depression, and substance use for craving management. This device can also be paired with counseling sessions.

This is the acute care room. This is where a patient who comes in an acute emergency is attended. We have all the emergency drugs that are standard for every hospital. Along with the basic first aid, we also have the NS, DNS, and Electrocardiogram (ECG), which is primarily essential for all patients before admissions.

This is the Ketamine infusion, one of the latest modalities in managing depression, OCD, and substance cravings for heroin and cocaine. We take a specific dose based on the patient’s weight and then dilute it in the normal saline. The solution is slowly infused via IV. It is not available at most rehab centres.
This is one of the best Transcranial Direct Current Stimulation device (TDCS). It not only has a role in depression treatment, it also plays a key role in addiction or craving management for substances like alcohol, cocaine, and heroin.
This is the first device I had procured and had become known for. We also have an infusion pump and monitor.
I will now take you to the IPD.
Access to the IPD area is completely secure. The doors of the IPD area are kept locked so they cannot escape. This has been done to ensure the safety of the patients. Every open area is covered with grills from all sides.
The other thing unique about the facility is that the lift has secured access to all the floors. Other than an authorised person with an ID card or the passcode, nobody can access the lift.
There’s also a doctor’s duty room if in case I need to stay back. We also have a ‘Happy Room.’

The Happy Room concept was created to encourage patients to spend time together and do some activities or play games. There are no television sets in the patients’ rooms because I wanted to encourage community participation. If they’re going to watch a match or movie, they can watch it together. The Happy Room is also used as the dining area.
For leisure activities, we have many board games and we also arrange Tambola every Sunday. There are also various books for them to read and spend some time in solitude. We offer art therapy as well.
We only have one public restroom in the facility that is attached to the Happy Room.
We have our own kitchen where food is prepared for the patients. I make sure that the facility is always absolutely clean.
We have a nursing station. There is a sink beside the procedure room so if a surgeon wants to wash their hands, they can.

This is IPD counselling or the rounds room where therapy is conducted for all patients.

Psychiatry is primarily known for Electroconvulsive Therapy or Traditional Electroshock Therapy. This device is used for patients with treatment-resistant schizophrenia and acute depression but not used for substance use.
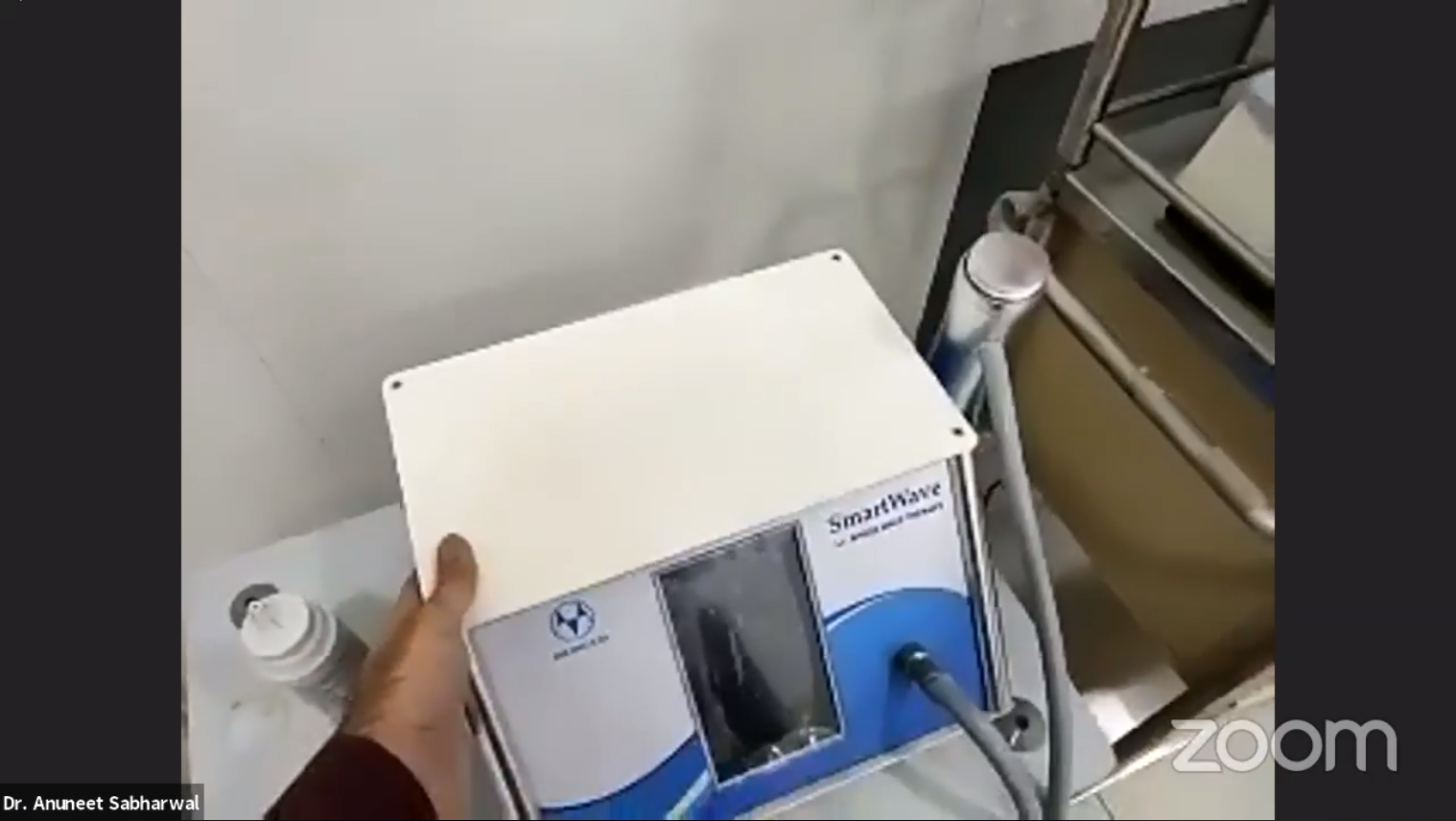
We also have a device known as the Extracorporeal Shockwave Therapy device, one of the latest modalities to manage erectile dysfunction. All the devices we have are cutting edge and top quality.
I will now take you to the area that all the patients will be interested in seeing. Apart from this, I will also give you a run-through of the ward.
We have this common area for the patients to relax. We do not have any ceiling fans but only wall fans. We adopted it as an anti-suicidal measure.
A patient got who got discharged today said she would have tried to suicide if there were any ceiling fans in the facility. We took all these measures while constructing this facility.

This is a single room. We have kept our rooms basic as we want patients to spend more time in the Happy Room and less time in their own rooms. It is spacious, and all the rooms come with attached bathrooms. There is no difference in the design of the bathrooms for single, double, or triple rooms. The same also goes for the furniture.

This is the triple sharing room. All our rooms are air-conditioned properly. You may have noticed some subtle things like no curtains. It is a deliberate endeavour. All the windows in the rooms have privacy films so that nothing is visible from outside during the day. However, everything is visible from outside at night.
A person is surrounded by people during the daytime and is unlikely to indulge in inappropriate behaviour. However, the same person will be doubly cautious since there are no curtains, and everything is visible from the outside. We also have spacious personal cabinets for each patient, including the bed storage section.
Vikram: What is the total number of beds in your facility?
Dr Sabharwal: We have 29 beds in the facility, of which two are single rooms, five triple rooms, and the remaining double rooms.
Vikram: How many of these rooms are occupied?
Dr Sabharwal: We have only recently started this facility. The third floor is also identical to this floor, where two patients are currently staying.
It was essentially meant to be a male-only facility, but our first two patients were females. Therefore, we have a policy for female patients to stay with an attendant at all costs. We do not allow any female patient to stay alone, as most of our staff are male.
It has almost been two months operating this facility. We started it on my son’s birthday, which was on August 28. I will show you how the facility looks from outside. It is an open and spacious area. You will not feel like a rehab centre here, but more like a relaxed hospital.
This is all about the hospital. I will now take you back to my chamber so that we can continue talking.
Vikram: I remember speaking to you in one of our earlier sessions in July about relapsing. Probably, it is already happening or bound to happen very soon. Apart from all this, if you can share a few things on how you took this challenging job of building a new setup during the COVID-19 pandemic?
Dr Sabharwal: The biggest challenge I faced was the labour not showing up at work as everything was under lockdown. The government had allowed non air polluting construction work to happen as long as the labourers stay in the facility. So, I let the labourers stay here during construction. It is how I managed to get the things done; otherwise, it would have taken another year to finish.
Other than this, my OPD was down and out. No patients were coming in, and there were no queries. It was also a massive challenge. But you have to take risks in life. I took the leap of faith to start this facility. I believed that this space would run.
Vikram (Question from Participant): You showed us many devices, but we won’t be able to remember the names. We see standard devices like pulse oximeter and BP monitor at all facilities. Are there any such devices for mental health as well?
Dr Sabharwal: There are such devices, but they are not legal in India for personal use. There are legal issues because only mental health professionals who hold a license use it. It is not available openly. For the moment, your best bet is to consult your psychiatrist. The things we have in this facility are not being used in India even by psychiatrists. Moreover, they may not be aware of all these devices.
Vikram: Please tell us about the different kinds of programmes you offer at The Happy Tree.
Dr Sabharwal: We have incredibly flexible programmes. If someone sends us a query through www.rehabs.in, they will immediately get a 41-page long handout on WhatsApp through the hospital’s number. This handout contains all the package details and programmes divided into procedures, psychotherapies, and bundles.
The charges are common for IPD and OPD. IPD differs only in the admission bundles that are 10-days, 20-days, and 30-days programmes. In most rehabs, we have 6-months long programmes, but we have taken a different approach to this and introduced these short-period programmes. The reason for doing this is – one: many people can not afford extremely high-quality care for six months – two: even those who can, do not want to spend six months in a centre where they have business issues and cannot meet people.
For these specific reasons, we have devices that combine counseling, medications, and brain stimulation to amplify treatment response to help patients get better quicker.
One thing I did not show during the tour is Naltrexone implants, which is also a rare thing. It never happens in rehabs, but we have introduced it at the lowest cost possible.
Naltrexone implants are used predominantly for heroin addiction, but they can be used for alcohol and other addictions as well.
When I talk about admission bundles, you look at the combination of these three. You also get additional discounts for taking them.
Our discounts are the same for everyone and transparent. We do not indulge in any differential pricing for patients, which most centres do. We function on a completely prepaid system and do not take admissions until the full amount for their stay has been deposited.
Our charges are also some of the cheapest you can find across all psychiatric hospitals, but the quality of care remains par excellence.
Vikram: How does insurance work at your facility?
Dr Sabharwal: We issue complete bills to the patients. They are free to claim the insurance as per will. The Indian government has made it mandatory to cover mental illness under insurance, but it does not yet apply to substance use. It is not mandatory for insurance companies to cover substance use. Even if the patient applies for the claim, they don’t usually get it.
I have seen many rejections for the same. Many patients also don’t tell these insurance companies about their substance abuse problems as the policy premiums go up. It is in addition to the bill not being paid by the insurance company.
Vikram: If I become an addict at some point in time and try to get insurance for my treatment, the insurance amount will be high at that point in time. Will it be wise for me to get insurance for mental health and addiction right now when I am not an addict but may develop the addiction later?
Dr Sabharwal: Mental health and addiction are two different things. Insurance companies right now are not covering substance use or any form of addiction. They cover mental health issues. I have never seen a company reimburse a patient for their substance use bills.
Most rehabs in the USA follow cash-only practices. I’m sure the founder of your organisation would also know. Most good high-quality rehabs are essentially cash-only setups. The setup of our quality and level in the US would also essentially be a cash-only facility.
Vikram: Do you only admit patients who are very serious and can’t take care of themselves, or you extend this facility to others as well?
Dr Sabharwal: Hospital has two roles – it can manifest as an end destination where the patient gets better, leaves the substance, discharges from the hospital, and goes home to continue with home-based relapse prevention.
The other option is that it essentially becomes an area of transition from here to a long facility. If you are administering all these brain stimulation procedures, it must be done in a medically supervised environment. It cannot be done randomly at a place where no medical supervision is available.
Our focus is to help the patient so much that they do not feel the need to visit a rehab. But should they need to go to rehab after a month, that place essentially works as a place of transition where they take the help they need. If you take the route where you visit a psychiatric hospital, detoxify, complete the initial rehabilitation, and then move to rehab, your recovery chances are two to three times higher.
Vikram: What kind of patients need 10-days, 20-days, or 30-days programmes?
Dr Sabharwal: A 10-days programme patient would essentially be someone who needs more intensive psychotherapy and less brain stimulation, along with medicines used for craving medicines. For instance, if I had a binge drinking patient, they would be kept on medications from day 1. Binge drinking patients do not have withdrawal symptoms per se, so these patients would be on daily psychotherapy sessions for 10-days. They can have assisted psychotherapy sessions with brain stimulation procedures. Binge drinking patients do not need detoxification
For patients who have alcohol withdrawal issues, irrespective of their dependence level, a 20-days minimum is essential because the detoxification takes at least a week. It is only after detoxification that we can initiate other procedures.
For people considering a Naltrexone implant, they cannot leave before 30-days. It can extend from 30 to 50 days as well. Because before administering an implant, we have to flush out substances from the person’s body with detoxification. Then we have to introduce Naltrexone orally for at least five to ten days. This is the time when the patient gets ready for an implant. The implant itself is shipped from Portugal and takes around 15 days to arrive. Meanwhile, the patient starts to get brain stimulation and psychotherapy.
The 10-days programme is essentially detoxification, whereas the 20-days programme is a combination of detoxification and ultra-short rehabilitation. The 30-days programme is detoxification and short rehabilitation.
Vikram (Question from Participant): Have you seen any difference between the patients before and after COVID-19? Is there any visible effect?
Dr Sabharwal: I have patients who have post-COVID anxiety, which is on the rise. I have seen a massive jump in anxiety in patients who either have had COVID or know someone who had it or someone who had died from it. If you ask about whether their substance use pattern has changed; with COVID, they were unable to source their substances initially, but now it is all available.
That is the reason why I mentioned earlier that relapse would happen once the lockdown is over. It is precisely what we see now.
Vikram (Question from Participant): Does your facility have brain stimulation therapies? If yes, are they similar to VNS and DBS?
Dr Sabharwal: In this facility, we have non-invasive procedures. DBS or Deep Brain Stimulation and VNS or Vagus Nerve Stimulation are invasive brain stimulation procedures performed by neurosurgeons. However, non-invasive procedures are performed by a psychiatrist.
VNS and DBS have not yet shown promising results for addiction. They are used for Parkinson’s, depression, and the likes but do not have evidence in substance use per se. If you want to get VNS and DBS done, it will be better to go to a neurosurgeon attached to a neurosurgery hospital.
Vikram: What are the legalities of the patients’ privacy rights who get admission to your facility for addiction?
Dr Sabharwal: It is not covered under the Mental Healthcare Act, 2017. In our psychiatric hospital, every single room has a camera except washrooms. We make this clear to our patients at the start about the cameras so that they remain behaved.
It is essential for patient safety purposes, as we have to keep track of not risking substance use in the facility.
Vikram: I agree. The life of a person is more important than their privacy. Is there any message you would like to share with us?
Dr Sabharwal: If you are using a substance, don’t feel shy to tell your family about it. Get the help you need. Trust me, professional help is massively different than taking help from friends and family. If you think you need professional help, do it right now. Do not wait for things to get worse, and do not wait to overdose.
If you have any other substance abuse problem, get help as fast as you can. Go to your nearest psychiatrist or a rehab centre and get the help you need. All the rehabilitation centres are open.
For more webinars like this, follow us on Facebook.
Reviewed by

Rajnandini Rathod
M.Sc. Psychology,Research Associate at RehabPath
Rajnandini is a psychologist and writer committed to making mental health knowledge accessible. With over five years of experience, she specializes in translating research into evidence-based, easy-to-understand content. Her PhD research focuses on mental health literacy and bridging the gap between awareness and support. She also works with individuals facing self-esteem issues and anxiety using a trauma-informed approach.













